This article examines mast cell activation through a systems homeostasis lens, emphasizing signal resolution, regulatory control, and clinical restraint.
Mast cell activation is a normal immune process.
Mast Cell Activation Syndrome represents something different: a failure of signal termination.
This distinction matters.
Activation vs Dysregulation
Mast cells are designed to respond to threat and then return to baseline. In MCAS, activation becomes persistent, amplified, and poorly regulated—often independent of the original trigger.
This does not mean mast cells are broken. It means the system has lost its ability to resolve signaling.
⏩ How MCAS Differs From Histamine Intolerance
Histamine intolerance reflects a mismatch between load and degradation capacity
MCAS reflects ongoing activation even when load is reduced
In MCAS, mast cells respond not only to antigens, but to neuro-immune signaling, endothelial stress, and metabolic strain.
This explains why MCAS presentations are multi-systemic, unpredictable, and poorly explained by food lists alone.
The Risk of Over-Diagnosis
Labeling reactive patients as having MCAS prematurely can freeze clinical reasoning, discourage recovery expectations, and promote lifelong suppression strategies.
MCAS is real—but it is not common, and it should not be the default explanation for histamine reactivity.
A Systems-Based Clinical Perspective
In many cases, mast cell behavior improves when:
⏩ barrier integrity is restored
⏩ immune load decreases
⏩ nervous system tone stabilizes
⏩ metabolic capacity improves
When activation persists despite these corrections, MCAS deserves careful evaluation—not reflex labeling.
Ethical Framing Matters
Not all activation is pathology.
Not all persistence is permanent.
Clinical precision requires both caution and restraint.
Systems Reminder
Persistent activation reflects failure of resolution—not necessarily irreversible disease.
✴️ How I Work
I work from a systems physiology perspective, looking at how environmental signals, nutrition, stress, digestion, and recovery interact to shape adaptive capacity—rather than chasing isolated symptoms.
Most conversations about health focus on nutrition, supplements, exercise, and stress.
But one of the most powerful—and most overlooked—inputs shaping human physiology is light.
Not light as brightness.
Not light as convenience.
But light as biological information.
Modern humans live in environments that are visually bright yet biologically incomplete. We spend most of our days under artificial lighting that looks adequate to the eye but lacks critical wavelengths present in natural sunlight—particularly near-infrared (NIR) and ultraviolet (UV) light.
This mismatch matters far more than most people realize.
Light as a Primary Regulatory Signal
Light interacts with human biology at multiple levels simultaneously:
Mitochondrial function (energy production and redox balance)
Neuroendocrine regulation (stress responsiveness and recovery)
Immune signaling (inflammatory tone and repair capacity)
The eye is not merely a visual organ—it is a regulatory interface that communicates environmental conditions directly to the brain and peripheral tissues.
When light signals are distorted, incomplete, or mistimed, downstream systems adapt accordingly.
The Problem with Modern Lighting
Most LED lighting is optimized for:
Energy efficiency
Visual brightness
Cost reduction
It is not optimized for human biology.
LEDs emit a narrow spectral range dominated by blue light, while lacking:
Near-infrared wavelengths that support mitochondrial signaling
The natural spectral balance found in sunlight and firelight
The result is an environment that can appear “bright” while being biologically disruptive—especially when exposure is prolonged and poorly timed.
Why This Matters at the Systems Level
When light signaling is chronically mismatched:
Circadian rhythms lose coherence
Stress signaling becomes exaggerated
Recovery and repair capacity decline
Metabolic flexibility narrows
Tolerance to other inputs (diet, exercise, supplements) decreases
In systems physiology, this is not viewed as a single problem—it is understood as background load that quietly shapes how all other systems respond.
No supplement can fully compensate for a mismatched environment.
A Note on Red Light, NIR, and Advanced Light Therapies
Targeted light exposures (including red and near-infrared wavelengths) are increasingly explored for their ability to influence cellular signaling and recovery pathways. These approaches are best understood not as treatments, but as contextual inputs that may support adaptive capacity when used appropriately and in the right sequence.
As with all physiological inputs, context, timing, and total load matter more than intensity.
How I Work
My work is grounded in systems physiology and signal integration.
Rather than isolating symptoms or chasing single mechanisms, I look at how multiple inputs—light, nutrition, stress, digestion, immune signaling, and recovery—interact to influence overall adaptive capacity.
This approach applies equally to:
Individuals navigating complex, persistent health challenges
Clinics and companies developing supplements or functional products intended to work with human physiology, not against it
The goal is coherence, not stimulation.
Final Thought
Before adding another intervention, it’s worth asking a simpler question:
Is the environment supporting the biology—or quietly working against it?
Light is not optional information.
It is foundational context.
Work With Me
Clinical Consulting
For individuals and practitioners seeking guidance grounded in systems homeostasis, adaptive capacity, and physiological regulation—not symptom chasing—my clinical services are available at:
OptimumHealthConsulting.com
Formulation & Product Development
If you are a clinic, practitioner, or company developing nutritional supplements, botanicals, or functional products, I provide formulation strategy and development grounded in systems physiology and real-world clinical application:
This article approaches chronic dysfunction through a systems homeostasis lens, emphasizing stress physiology, neuroendocrine regulation, and downstream tissue tolerance rather than isolated organ-based causality.
A Systems Perspective on Stress, Regulation, and Downstream Dysfunction
It’s increasingly common to hear the phrase: “All health and disease start in the gut.”
This view exists for good reason. The gastrointestinal system is central to digestion, immunity, inflammation, and nutrient assimilation. It is richly innervated, metabolically demanding, and highly responsive to environmental inputs. When systems are under strain, the gut is often one of the first places dysfunction becomes visible.
But visibility is not the same as origin.
From a systems homeostasis and neuroendocrine perspective, chronic dysfunction rarely begins in the gut. More often, it begins with stress signaling and loss of regulatory control, with gastrointestinal dysfunction emerging downstream.
Why the Gut Often Appears to Be the Starting Point
The gut is uniquely sensitive to systemic stress because it is:
highly dependent on autonomic balance
energetically expensive to maintain
tightly coupled to immune signaling
responsive to circadian and neuroendocrine regulation
When stress physiology becomes chronic, digestive capacity, motility, barrier integrity, and immune tolerance are among the first functions to degrade.
This makes the gut an excellent early indicator of dysregulation — but not necessarily the primary driver.
Stress as the Upstream Signal
In a systems-based model, stress precedes dysfunction.
Stress here is not limited to psychological stress. It includes:
perceived threat
sleep disruption
metabolic strain
inflammatory load
under-recovery
circadian mismatch
These stressors converge on the HPA axis, autonomic nervous system, and neuroimmune signaling, altering how energy is allocated, how barriers are maintained, and how inflammation is resolved.
As regulatory capacity declines, gastrointestinal function adapts accordingly — often by reducing digestive output, increasing permeability, and activating immune defenses.
When Treating the Gut Alone Falls Short
When dysfunction is assumed to start in the gut, practitioners may:
over-target gastrointestinal findings
escalate protocols based on lab abnormalities
miss upstream drivers of reduced tolerance
unintentionally increase total system load
In these cases, improving gut markers does not reliably translate into improved clinical outcomes — not because gut work is misguided, but because the system driving the dysfunction has not been addressed.
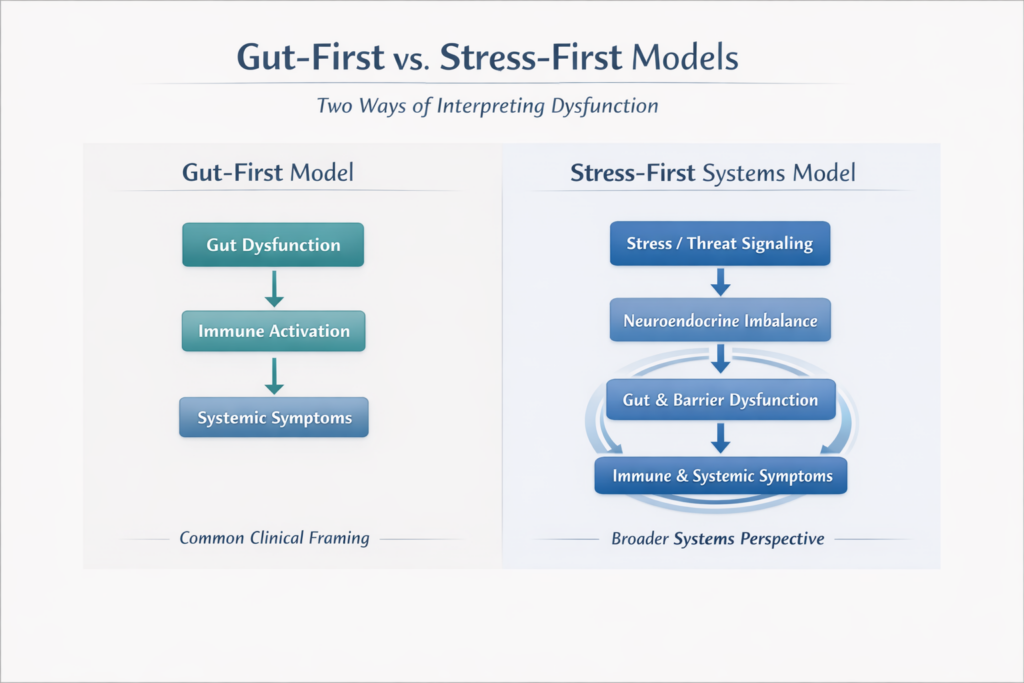
A More Accurate Systems Sequence
From a neuroendocrine systems perspective, dysfunction more often follows this pattern:
Stress / Threat Signaling
→ Neuroendocrine Dysregulation
→ Autonomic Imbalance
→ Loss of Digestive Capacity
→ Barrier Dysfunction
→ Immune Activation
→ Systemic Symptoms
The gut is central — but it is not primary.
Why This Distinction Matters Clinically
Recognizing the gut as a downstream responder rather than the origin allows care to become:
better sequenced
less aggressive
more tolerable
more sustainable
Interventions shift from correcting findings to restoring regulatory capacity, often allowing gastrointestinal function to normalize as part of broader recovery.
Systems Reminder
You don’t treat where dysfunction appears.
You treat the system that made dysfunction necessary.
The gut tells an important story — but it is rarely the first chapter.
How I Work
I approach clinical and formulation work through a systems homeostasis framework, prioritizing stress physiology, regulatory capacity, and intervention tolerance before targeting downstream findings. This sequencing supports recovery rather than overwhelming already stressed systems.
Selected References
Mayer EA et al. The gut–brain axis: interactions between stress, neuroendocrine signaling, and gastrointestinal function. Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/37756251/
This article approaches gastrointestinal, immune, and neurological reactivity through a systems homeostasis lens—focusing on regulation, tolerance, and recovery rather than symptom suppression or isolated mechanisms.
Why “Histamine Intolerance” Is Usually a Barrier and Regulation Disorder
Histamine intolerance is increasingly common in integrative and functional medicine practices. Individuals present with food reactions, flushing, headaches, anxiety, gut symptoms, rashes, palpitations, or a sense that “everything triggers me now.”
The usual explanations focus on food lists, genetics, or histamine suppression. While these approaches can reduce symptoms temporarily, they often fail to explain why tolerance was lost in the first place.
From a systems homeostasis perspective, histamine intolerance is rarely a primary histamine problem. It is most often a barrier, degradation, immune, and nervous system regulation problem.
Histamine Is a Normal Signal, Not a Toxin
Histamine is an essential signaling molecule involved in immune surveillance, gastric acid secretion, vascular tone, neurotransmission, and tissue repair.
In a regulated system, histamine rises and falls appropriately and is rapidly degraded. Problems arise not because histamine exists, but because clearance and resolution fail to keep pace with signaling load.
DAO: Degradation Capacity, Not a Cure
Diamine oxidase (DAO) is the primary enzyme responsible for degrading luminal histamine in the gut. It is produced by healthy enterocytes and functions as a first-pass clearance mechanism.
DAO capacity is reduced by intestinal inflammation, mucosal injury, oxidative stress, impaired nutrient status, and loss of epithelial integrity.
DAO supplementation can reduce symptoms, but it does not resolve the upstream reason DAO production declined. When used as a permanent strategy, it often masks barrier failure rather than correcting it. DAO is best understood as temporary load management, not resolution.
Zonulin and Barrier Regulation
Zonulin regulates intestinal tight junctions and therefore permeability. Elevated zonulin reflects loss of barrier control, allowing luminal antigens to interact with the immune system.
This has two critical consequences:
Immune activation increases histamine release
DAO production declines as enterocyte health deteriorates
Barrier dysfunction therefore both raises histamine signaling and reduces histamine clearance at the same time.
Mast Cells: Effectors, Not the Root Cause
Mast cells are highly sensitive immune sentinels concentrated at barrier surfaces. In a regulated system, mast cell activation is precise, proportional, and self-resolving.
In dysregulated systems, mast cells become chronically reactive—not because they are defective, but because the environment remains threatening.
Drivers of mast cell overactivity include:
barrier disruption
persistent immune signaling
impaired histamine degradation
nervous system threat signaling
Mast cells are responding appropriately. The system is failing to resolve the signal.
Nervous System Signaling and Histamine Reactivity
Mast cells express receptors for stress-related neuropeptides such as CRH and substance P. Chronic stress, sympathetic dominance, and low vagal tone lower the activation threshold for mast cell degranulation.
This explains why symptoms flare with stress, feel unpredictable, and often improve when the system is calmed—even before laboratory markers normalize.
Histamine intolerance is therefore both an immune and a neuro-regulatory phenomenon.
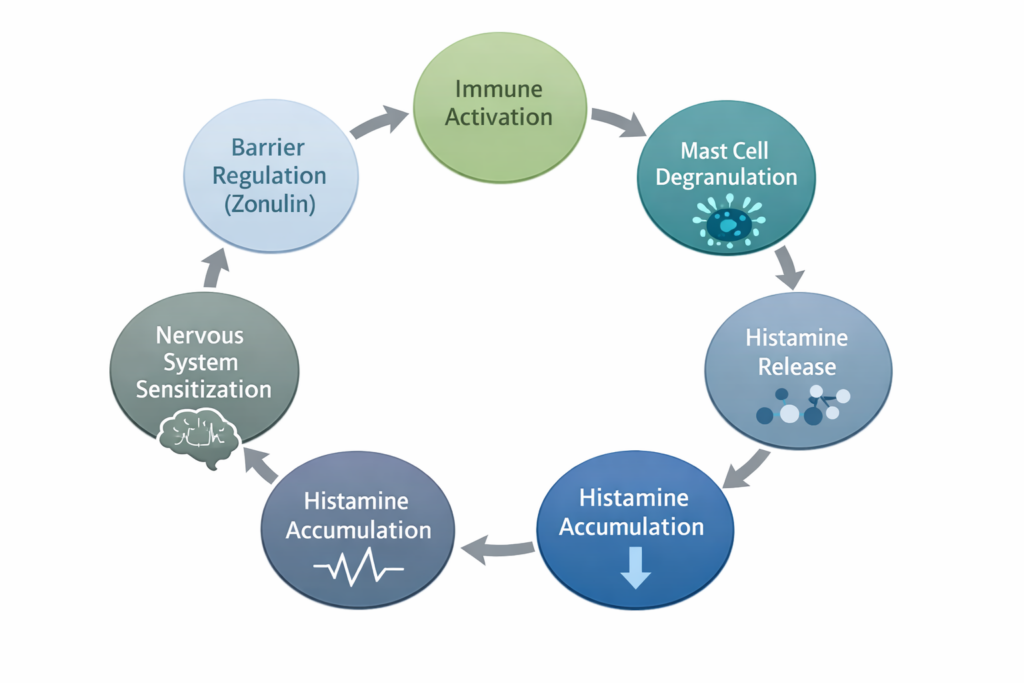
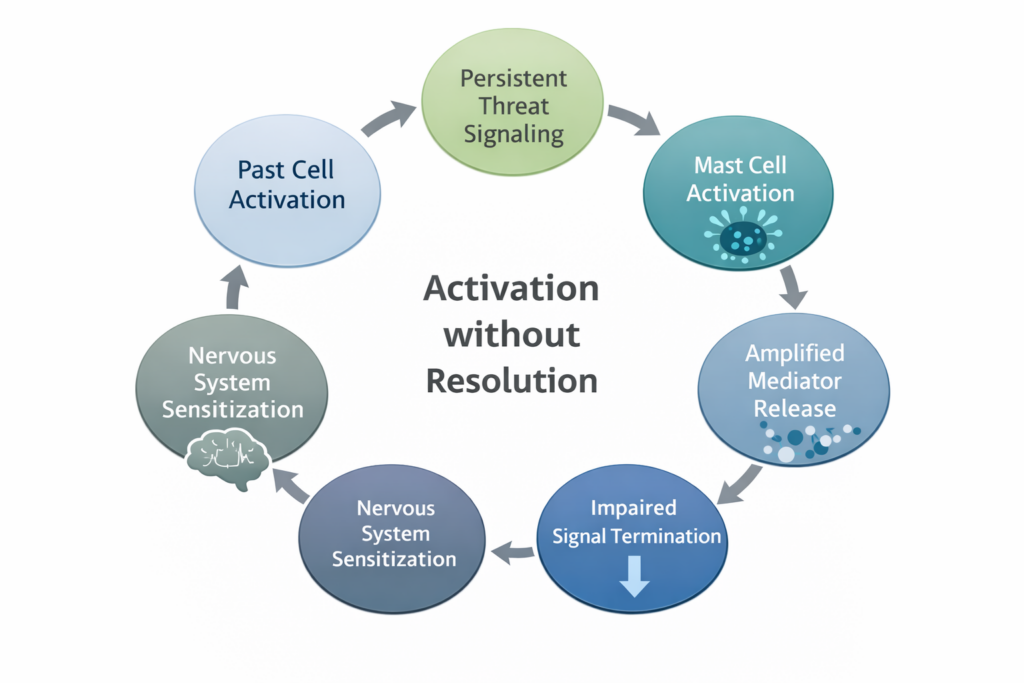
The Systems Loop
Taken together, the pattern is clear:
Barrier disruption (zonulin)
→ immune activation
→ mast cell degranulation
→ histamine release
→ reduced DAO clearance
→ histamine accumulation
→ nervous system sensitization
→ further mast cell activation and barrier stress
Suppressing one node shifts load elsewhere. Resolution requires restoring regulation.
Why Food Avoidance and DAO Alone Fail
Low-histamine diets and DAO supplementation reduce incoming load but do not restore barrier integrity, normalize immune tone, rebuild enzymatic capacity, or recalibrate nervous system signaling.
Over time, restriction often reduces resilience further, reinforcing sensitivity instead of restoring tolerance.
A note on Mast Cell Activation Syndrome (MCAS)
It’s important to distinguish between mast cell overactivity within a dysregulated system and true mast cell activation syndromes.
Many individuals experiencing histamine intolerance do not have primary mast cell disease. In these cases, mast cells are responding appropriately to unresolved immune, barrier, and nervous system threat signals.
There are, however, situations where mast cell activation becomes persistent and poorly regulated, requiring a different level of clinical consideration. Because this distinction matters—both clinically and ethically—a separate article will follow examining Mast Cell Activation Syndrome (MCAS) through a systems homeostasis lens.
Systems Reminder
Interventions only work when the system has the capacity to tolerate them.
DAO reduces histamine load.
Tolerance returns only when barrier regulation, immune signaling, and nervous system tone are restored.
How I Work
I approach health, formulation, and clinical decision-making through a systems homeostasis framework, prioritizing capacity, tolerance, recovery, and regulation before escalation. Rather than chasing symptoms, markers, or isolated pathways, I focus on sequencing interventions so the system can safely respond instead of being overwhelmed.
Lion’s Mane mushroom has become one of the most talked-about “brain health” ingredients—often framed as a way to boost BDNF, rewire the brain, or even reverse cognitive decline.
The problem isn’t that Lion’s Mane has no value.
The problem is that most discussions ignore systems context.
Lion’s Mane is best understood not as a brain-rewiring agent, but as a neurotrophic signal modulator whose effects depend entirely on system readiness.
What Makes Lion’s Mane Biologically Interesting?
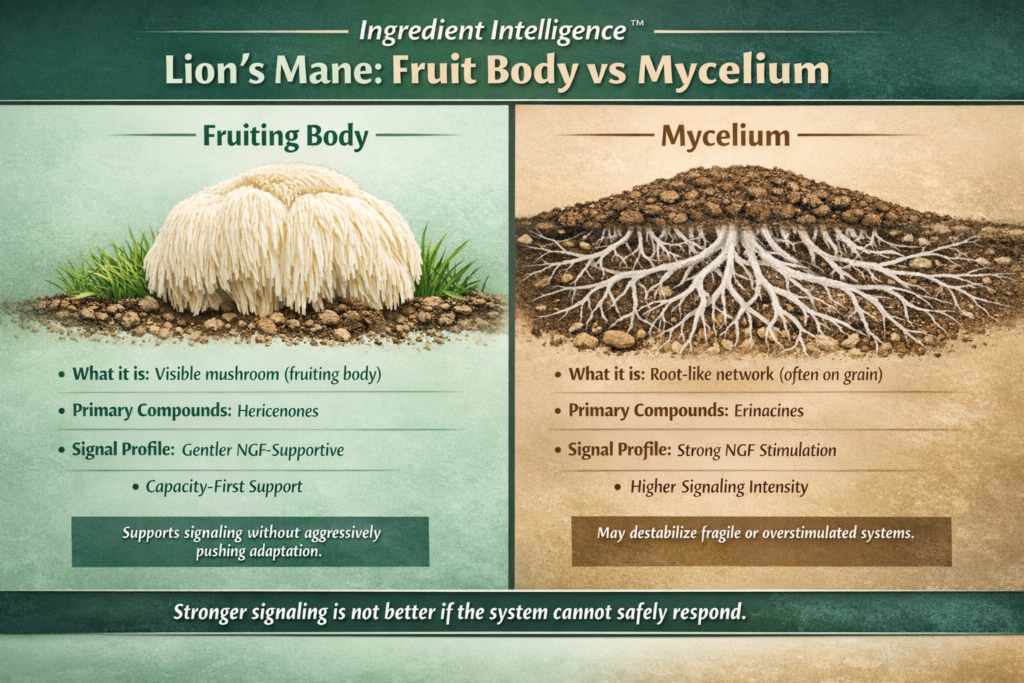
Lion’s Mane contains two main classes of bioactive compounds:
Hericenones – primarily found in the fruiting body
Erinacines – primarily found in the mycelium
Both have been shown—mostly in preclinical research—to stimulate nerve growth factor (NGF) signaling. NGF operates within the same neurotrophic ecosystem as BDNF, supporting neuronal maintenance, learning, and adaptation.
What matters clinically is not whether a signal exists—but whether the system can safely respond to it.
Fruiting Body vs Mycelium: Why the Difference Matters
Fruiting Body (the visible mushroom)
Richer in hericenones
Traditionally consumed as food
Generally associated with gentler neurotrophic signaling
Lower risk of grain contamination when properly grown
Systems interpretation:
Fruiting body–dominant extracts tend to provide context-dependent support that aligns better with capacity-first, non-overstimulating use.
Mycelium (the underground network)
Richer in erinacines
Commonly grown on grain substrates
May deliver stronger neurotrophic signals
Requires careful extraction to avoid excess starch
Systems interpretation:
Mycelium-derived products can push stronger signaling, which may only be appropriate in systems with stable energy, sleep, and recovery capacity. In fragile or overstimulated systems, this can backfire.
Stronger signaling is not better if the system cannot safely respond.
What the Human Research Actually Shows
Small human trials in individuals with mild cognitive impairment (MCI) have shown:
Modest improvements in cognitive test scores
Loss of benefit after discontinuation
This is a crucial but often ignored detail.
When benefits disappear after withdrawal, the intervention is likely supportive rather than transformative—participating in signaling, not inducing durable structural change.
Signals require safety, energy availability, sleep, and repetition to translate into function
You can increase neurotrophic signaling in a system that lacks capacity—and worsen outcomes.
This explains why some individuals experience:
anxiety
brain fog
sleep disruption when aggressively “stimulating” the nervous system without adequate recovery.
Where Lion’s Mane May Be Appropriate
Lion’s Mane may be contextually useful when:
Cognitive symptoms fluctuate with stress and recovery
Sleep, metabolic stability, and energy availability are already solid
The nervous system is not in a fragile or depleted state
In these cases, Lion’s Mane functions as a signal supporter, not a repair mechanism.
Where Lion’s Mane Is Commonly Misused
Lion’s Mane is often overapplied when:
Neuroinflammation or structural pathology is active
Sleep debt or metabolic instability is unresolved
The system is already overstimulated
In these contexts, “boosting neuroplasticity” can increase instability rather than resilience.
Canonical Ingredient Intelligence™ Takeaway
Neuroplasticity follows readiness—it cannot be forced.
Lion’s Mane does not “rewire the brain.”
It participates in neurotrophic signaling when the system can safely respond.
That distinction separates clinical reasoning from marketing.
Ingredient Intelligence™ Summary
Lion’s Mane supports neurotrophic signaling, not guaranteed neurogenesis
Effects appear context-dependent and reversible
Fruiting body and mycelium are not interchangeable
BDNF reflects system readiness, not inevitability
This ingredient makes sense only when viewed through a systems homeostasis lens.
Interventions only work when the system has the capacity to tolerate them—otherwise even “good” inputs can destabilize the whole.
How I work: I approach health, formulation, and clinical decision-making through a systems homeostasis lens—prioritizing capacity, tolerance, recovery, and regulation before escalation. Rather than chasing symptoms or markers, I focus on sequencing interventions so they support stability instead of overwhelming the system.
Clinical & Formulation Context
Formulation / Product Development
If you are a clinic, practitioner, or company developing nutritional supplements, botanicals, or functional products, I provide formulation strategy and development grounded in systems physiology and real-world clinical application.
HealthspanFormulations.com
Clinical Consulting
For individuals and practitioners seeking clinical consulting rooted in systems homeostasis, metabolic regulation, and adaptive capacity—not symptom chasing—my clinical services are available at:
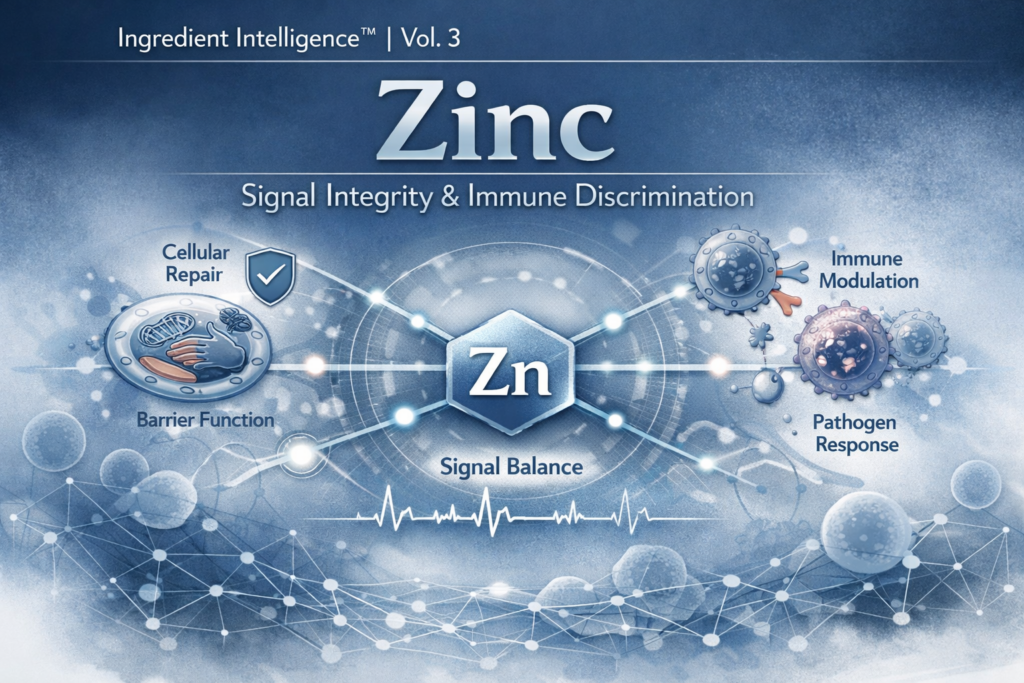
That framing explains why zinc is frequently misunderstood — and frequently misused.
Zinc does not push physiology forward.
It calibrates how systems respond.
From a systems homeostasis perspective, zinc functions as a regulator of signal integrity. It sits at the intersection of immune signaling, tissue repair, transcriptional control, and barrier function — not to amplify responses, but to ensure they are appropriate, proportional, and resolvable.
When zinc availability is sufficient, communication between systems is clear. When it is not, signaling becomes noisy, exaggerated, or poorly coordinated.
What Zinc Insufficiency Looks Like Systemically
Zinc insufficiency rarely presents as a single, obvious deficiency. Instead, it often appears as patterns of reduced tolerance:
slower tissue repair
impaired barrier integrity
blunted or dysregulated immune responses
reduced resilience under physiological stress
These patterns reflect loss of coordination, not lack of force.
The Hidden Trade-Off
Because zinc supports immune and repair pathways, it is often assumed that more zinc equals better protection. In practice, chronic zinc loading can distort signaling balance, interfere with complementary mineral systems, and reduce long-term resilience.
Zinc does not reward excess.
It rewards precision and context.
Zinc Through a Systems Homeostasis Lens
Within systems homeostasis, zinc acts as a boundary regulator — helping determine:
when immune activation is appropriate
when repair should proceed
when signaling should resolve
In low-reserve systems, zinc mismanagement can amplify fragility rather than restore resilience. Its value depends entirely on energetic context, inflammatory load, and recovery capacity.
Closing Principle
Zinc strengthens systems not by pushing them harder, but by helping them respond appropriately.
When resilience is the goal, signal integrity matters more than stimulation.
Clinical & Professional Context
This systems-based framework reflects the same approach used in both clinical practice and professional consulting.
Clinical services: OptimumHealthConsulting.com
OptimumHealthConsulting.com
If you’re a clinic, practitioner, or company interested in formulation strategy or systems-based ingredient design:

 OptimumHealthConsulting.com
OptimumHealthConsulting.com