Lion’s Mane mushroom has become one of the most talked-about “brain health” ingredients—often framed as a way to boost BDNF, rewire the brain, or even reverse cognitive decline.
The problem isn’t that Lion’s Mane has no value.
The problem is that most discussions ignore systems context.
Lion’s Mane is best understood not as a brain-rewiring agent, but as a neurotrophic signal modulator whose effects depend entirely on system readiness.
What Makes Lion’s Mane Biologically Interesting?
Lion’s Mane contains two main classes of bioactive compounds:
- Hericenones – primarily found in the fruiting body
- Erinacines – primarily found in the mycelium
Both have been shown—mostly in preclinical research—to stimulate nerve growth factor (NGF) signaling. NGF operates within the same neurotrophic ecosystem as BDNF, supporting neuronal maintenance, learning, and adaptation.
What matters clinically is not whether a signal exists—but whether the system can safely respond to it.
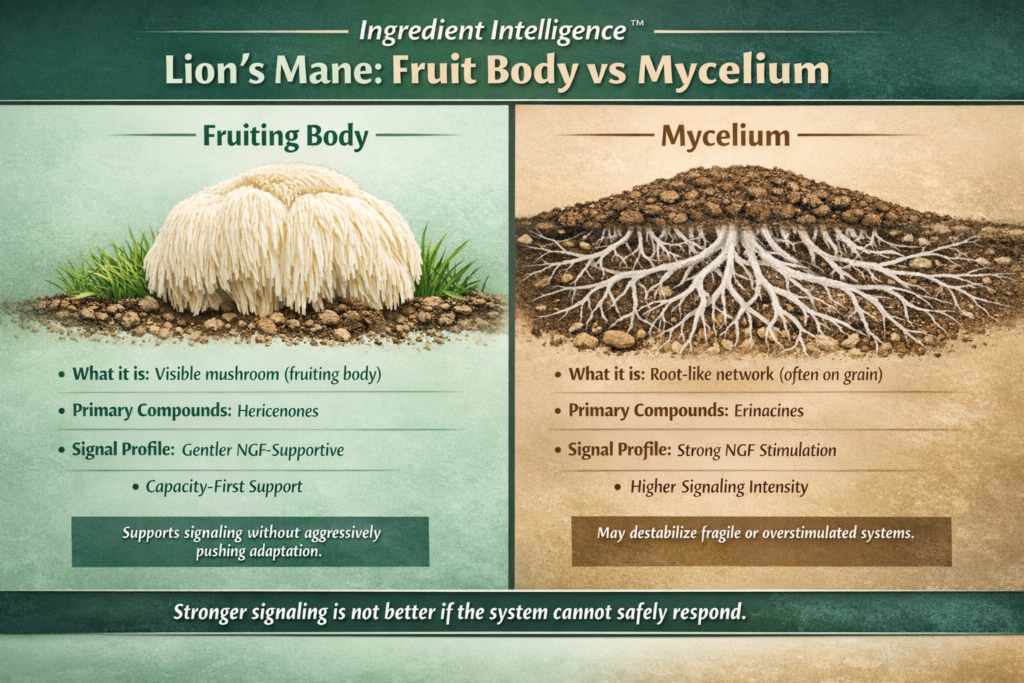
Fruiting Body vs Mycelium: Why the Difference Matters
Fruiting Body (the visible mushroom)
- Richer in hericenones
- Traditionally consumed as food
- Generally associated with gentler neurotrophic signaling
- Lower risk of grain contamination when properly grown
Systems interpretation:
Fruiting body–dominant extracts tend to provide context-dependent support that aligns better with capacity-first, non-overstimulating use.
Mycelium (the underground network)
- Richer in erinacines
- Commonly grown on grain substrates
- May deliver stronger neurotrophic signals
- Requires careful extraction to avoid excess starch
Systems interpretation:
Mycelium-derived products can push stronger signaling, which may only be appropriate in systems with stable energy, sleep, and recovery capacity. In fragile or overstimulated systems, this can backfire.
Stronger signaling is not better if the system cannot safely respond.
What the Human Research Actually Shows
Small human trials in individuals with mild cognitive impairment (MCI) have shown:
- Modest improvements in cognitive test scores
- Loss of benefit after discontinuation
This is a crucial but often ignored detail.
When benefits disappear after withdrawal, the intervention is likely supportive rather than transformative—participating in signaling, not inducing durable structural change.
BDNF, Neuroplasticity, and a Common Mistake
BDNF is frequently treated as a control knob:
Increase BDNF → increase neuroplasticity → improve cognition
In reality:
- BDNF is a mediator, not a master switch
- Neuroplasticity is conditional
- Signals require safety, energy availability, sleep, and repetition to translate into function
- You can increase neurotrophic signaling in a system that lacks capacity—and worsen outcomes.
This explains why some individuals experience:
- anxiety
- brain fog
- sleep disruption when aggressively “stimulating” the nervous system without adequate recovery.
Where Lion’s Mane May Be Appropriate
Lion’s Mane may be contextually useful when:
- Cognitive symptoms fluctuate with stress and recovery
- Sleep, metabolic stability, and energy availability are already solid
- The nervous system is not in a fragile or depleted state
In these cases, Lion’s Mane functions as a signal supporter, not a repair mechanism.
Where Lion’s Mane Is Commonly Misused
Lion’s Mane is often overapplied when:
- Neuroinflammation or structural pathology is active
- Sleep debt or metabolic instability is unresolved
- The system is already overstimulated
In these contexts, “boosting neuroplasticity” can increase instability rather than resilience.
Canonical Ingredient Intelligence™ Takeaway
- Neuroplasticity follows readiness—it cannot be forced.
- Lion’s Mane does not “rewire the brain.”
- It participates in neurotrophic signaling when the system can safely respond.
That distinction separates clinical reasoning from marketing.
Ingredient Intelligence™ Summary
- Lion’s Mane supports neurotrophic signaling, not guaranteed neurogenesis
- Effects appear context-dependent and reversible
- Fruiting body and mycelium are not interchangeable
- BDNF reflects system readiness, not inevitability
This ingredient makes sense only when viewed through a systems homeostasis lens.
Interventions only work when the system has the capacity to tolerate them—otherwise even “good” inputs can destabilize the whole.
How I work: I approach health, formulation, and clinical decision-making through a systems homeostasis lens—prioritizing capacity, tolerance, recovery, and regulation before escalation. Rather than chasing symptoms or markers, I focus on sequencing interventions so they support stability instead of overwhelming the system.
Clinical & Formulation Context
Formulation / Product Development
If you are a clinic, practitioner, or company developing nutritional supplements, botanicals, or functional products, I provide formulation strategy and development grounded in systems physiology and real-world clinical application.
HealthspanFormulations.com
Clinical Consulting
For individuals and practitioners seeking clinical consulting rooted in systems homeostasis, metabolic regulation, and adaptive capacity—not symptom chasing—my clinical services are available at:
OptimumHealthConsulting.com
#IngredientIntelligence #LionMane #Neuroplasticity #BDNF #SystemsHomeostasis #Regulome #NutraceuticalInnovation #ProductFormulation #RobLamberton #RobertLamberton