Clinical Implications of the New USDA Dietary Guidelines
The most recent USDA Dietary Guidelines have again raised concern that increasing animal-based protein intake may elevate cardiovascular disease (CVD) risk due to associated saturated fat consumption.
While this concern remains common, it is increasingly inconsistent with current cardiovascular research.
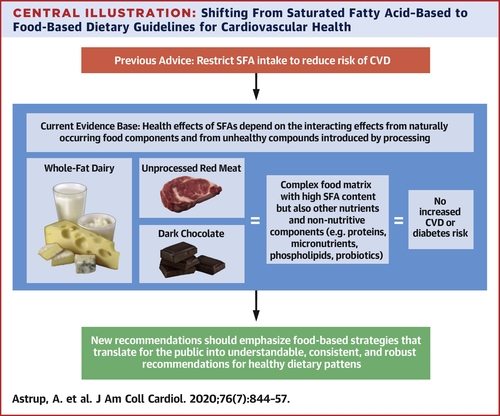
A comprehensive 2020 review published in the Journal of the American College of Cardiology—Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations—reexamined decades of epidemiologic, mechanistic, and interventional data. The authors concluded that saturated fat intake, in isolation, is a poor predictor of cardiovascular risk.
For clinicians, this distinction is highly relevant when interpreting dietary guidelines and counseling patients.
Limitations of LDL-C–Focused Risk Models
Current USDA guidance continues to emphasize saturated fat restriction largely through its impact on LDL cholesterol (LDL-C). However, the JACC review highlights a key limitation of this approach: LDL-C alone does not adequately reflect atherogenic risk.
More informative risk markers include:
- LDL particle number and density
- Insulin resistance and glycaemic regulation
- Chronic inflammatory burden
- Overall metabolic health status
Small, dense LDL particles—frequently associated with insulin resistance and hyperglycaemia—exhibit significantly greater atherogenic potential than large, buoyant LDL particles. Importantly, higher saturated fat intake within whole-food dietary patterns does not consistently produce this adverse lipid phenotype.
From a clinical standpoint, this challenges the assumption that saturated fat reduction should remain a primary target independent of metabolic context.
Historical Context and Policy Lag
The USDA’s continued caution regarding saturated fat reflects longstanding assumptions rooted in mid-20th-century observational research, particularly the Seven Countries Study led by Ancel Keys.
Subsequent evaluations have identified methodological limitations in this work, including selective data inclusion and insufficient control for confounding factors such as sugar intake, smoking prevalence, and lifestyle variables. More recent randomized trials and meta-analyses have not consistently replicated its conclusions.
Nevertheless, dietary policy has been slow to integrate newer mechanistic and clinical evidence.
Animal Protein: Clinically Relevant Distinctions
The USDA Dietary Guidelines largely categorize animal protein as a single entity. In clinical practice, this simplification obscures important distinctions.
Differences between:
- CAFO-raised animal foods, and
- Grass-fed, pasture-raised animal foods
extend beyond ethical considerations and include variations in fatty acid composition, micronutrient density, and inflammatory potential. These factors can meaningfully influence metabolic and inflammatory responses in patients.
Dietary Pattern and the Role of Fibre
Another limitation of saturated fat-focused guidance is the insufficient consideration of dietary pattern.
The JACC review emphasizes that saturated fat intake must be evaluated in conjunction with:
- Fibre intake
- Refined carbohydrate exposure
- Insulin sensitivity and metabolic health
Dietary fibre plays a central role in insulin regulation, gut microbial ecology, bile acid metabolism, and lipid handling. When saturated fat is consumed within a fibre-rich, minimally processed dietary pattern, lipid changes commonly associated with increased cardiovascular risk are often attenuated or absent.
This context is rarely reflected in public dietary guidance but is highly relevant in individualized clinical care.
Practical Implications for Clinicians
For practitioners, the implication of the new USDA Dietary Guidelines is not that saturated fat should be universally promoted or avoided, but that single-nutrient targets are insufficient for cardiovascular risk assessment.
The most consistent drivers of CVD risk remain:
- Insulin resistance
- Chronic inflammation
- Hyperglycaemia
- Sedentary behavior
- Ultra-processed food consumption
These factors are not caused by saturated fat intake alone and, in many cases, were exacerbated by decades of dietary guidance that encouraged refined carbohydrate substitution.
Conclusion
The renewed debate surrounding the USDA Dietary Guidelines highlights the need for a more physiologically grounded approach to cardiovascular nutrition—one that prioritizes metabolic health, dietary pattern, and food quality over isolated macronutrient thresholds.
The JACC review represents an important step toward that shift. For clinicians, incorporating this evidence into clinical reasoning may help reconcile public dietary policy with individualized patient care.
In Practice: Key Takeaways for Clinicians
- Evaluate cardiovascular risk in the context of metabolic health, not LDL-C alone
- Consider LDL particle characteristics, insulin resistance, and inflammation when assessing dietary fat intake
- Distinguish between animal food sources rather than treating all animal protein as metabolically equivalent
- Emphasize dietary pattern and fibre intake when discussing saturated fat with patients
- Avoid reflexive fat restriction in metabolically healthy individuals without additional risk markers
Reference
Journal of the American College of Cardiology (2020)
Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations
Clinical Implications of the New USDA Dietary Guidelines
The most recent USDA Dietary Guidelines have again raised concern that increasing animal-based protein intake may elevate cardiovascular disease (CVD) risk due to associated saturated fat consumption.
While this concern remains common, it is increasingly inconsistent with current cardiovascular research.
A comprehensive 2020 review published in the Journal of the American College of Cardiology—Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations—reexamined decades of epidemiologic, mechanistic, and interventional data. The authors concluded that saturated fat intake, in isolation, is a poor predictor of cardiovascular risk.
For clinicians, this distinction is highly relevant when interpreting dietary guidelines and counseling patients.
Limitations of LDL-C–Focused Risk Models
Current USDA guidance continues to emphasize saturated fat restriction largely through its impact on LDL cholesterol (LDL-C). However, the JACC review highlights a key limitation of this approach: LDL-C alone does not adequately reflect atherogenic risk.
More informative risk markers include:
- LDL particle number and density
- Insulin resistance and glycaemic regulation
- Chronic inflammatory burden
- Overall metabolic health status
Small, dense LDL particles—frequently associated with insulin resistance and hyperglycaemia—exhibit significantly greater atherogenic potential than large, buoyant LDL particles. Importantly, higher saturated fat intake within whole-food dietary patterns does not consistently produce this adverse lipid phenotype.
From a clinical standpoint, this challenges the assumption that saturated fat reduction should remain a primary target independent of metabolic context.
Historical Context and Policy Lag
The USDA’s continued caution regarding saturated fat reflects longstanding assumptions rooted in mid-20th-century observational research, particularly the Seven Countries Study led by Ancel Keys.
Subsequent evaluations have identified methodological limitations in this work, including selective data inclusion and insufficient control for confounding factors such as sugar intake, smoking prevalence, and lifestyle variables. More recent randomized trials and meta-analyses have not consistently replicated its conclusions.
Nevertheless, dietary policy has been slow to integrate newer mechanistic and clinical evidence.
Animal Protein: Clinically Relevant Distinctions
The USDA Dietary Guidelines largely categorize animal protein as a single entity. In clinical practice, this simplification obscures important distinctions.
Differences between:
- CAFO-raised animal foods, and
- Grass-fed, pasture-raised animal foods
extend beyond ethical considerations and include variations in fatty acid composition, micronutrient density, and inflammatory potential. These factors can meaningfully influence metabolic and inflammatory responses in patients.
Dietary Pattern and the Role of Fibre
Another limitation of saturated fat-focused guidance is the insufficient consideration of dietary pattern.
The JACC review emphasizes that saturated fat intake must be evaluated in conjunction with:
- Fibre intake
- Refined carbohydrate exposure
- Insulin sensitivity and metabolic health
Dietary fibre plays a central role in insulin regulation, gut microbial ecology, bile acid metabolism, and lipid handling. When saturated fat is consumed within a fibre-rich, minimally processed dietary pattern, lipid changes commonly associated with increased cardiovascular risk are often attenuated or absent.
This context is rarely reflected in public dietary guidance but is highly relevant in individualized clinical care.
Practical Implications for Clinicians
For practitioners and the general public, the implication of the new USDA Dietary Guidelines is not that saturated fat should be universally promoted or avoided, but that single-nutrient targets are insufficient for cardiovascular risk assessment.
The most consistent drivers of CVD risk remain:
- Insulin resistance
- Chronic inflammation
- Hyperglycaemia (high blood sugar)
- Sedentary behavior
- Ultra-processed food consumption
These factors are not caused by saturated fat intake alone and, in many cases, were exacerbated by decades of dietary guidance that encouraged refined carbohydrate substitution.
Conclusion
The renewed debate surrounding the USDA Dietary Guidelines highlights the need for a more physiologically grounded approach to cardiovascular nutrition—one that prioritizes metabolic health, dietary pattern, and food quality over isolated macronutrient thresholds.
The JACC review represents an important step toward that shift. For clinicians, incorporating this evidence into clinical reasoning may help reconcile public dietary policy with individualized patient care.
In Practice: Key Takeaways for Clinicians
- Evaluate cardiovascular risk in the context of metabolic health, not LDL-C alone
- Consider LDL particle characteristics, insulin resistance, and inflammation when assessing dietary fat intake
- Distinguish between animal food sources rather than treating all animal protein as metabolically equivalent
- Emphasize dietary pattern and fibre intake when discussing saturated fat with patients
- Avoid reflexive fat restriction in metabolically healthy individuals without additional risk markers
Reference
Journal of the American College of Cardiology (2020)
Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations
https://www.jacc.org/doi/full/10.1016/j.jacc.2020.05.077


 Compounding formulation (sterile & non-sterile)
Compounding formulation (sterile & non-sterile) Development of a 46-SKU botanical precision-medicine range
Development of a 46-SKU botanical precision-medicine range Operational systems & quality assurance integration
Operational systems & quality assurance integration Practitioner education programs in functional nutrition, integrative medicine, and metabolic assessment
Practitioner education programs in functional nutrition, integrative medicine, and metabolic assessment Clinical translation of regenerative and longevity protocols
Clinical translation of regenerative and longevity protocols