Preservatives are one of the great conveniences of modern life.
They allow food to travel farther, last longer, and remain visually appealing weeks or months after production. From a supply-chain perspective, they solve real problems.
From a biological perspective, however, preservatives are not neutral.
They are chemical inputs that interact with living systems — particularly the gut, immune system, and cellular energy machinery. And when exposure is frequent, layered, and begins early in life, those interactions matter.
The image above illustrates a systems-based reality that is increasingly difficult to ignore.
Preservatives Don’t Act in Isolation
Most discussions about preservatives focus on individual safety thresholds:
“Is this ingredient approved?”
“Is it below the allowable daily intake?”
Those questions are necessary — but insufficient.
Biology doesn’t experience ingredients one at a time.
It experiences total exposure.
Children today are exposed to preservatives across:
Packaged foods and snacks
Beverages
Condiments and sauces
Medications
Supplements
Each exposure may be small. The cumulative biological load is not.
The Gut: First Contact, First Consequence
The gastrointestinal tract is the primary interface between preservatives and the body.
Many preservatives are antimicrobial by design. While this helps prevent spoilage, it also means they can influence the gut ecosystem — especially with repeated exposure.
Even subtle shifts in gut ecology can affect:
Microbial diversity
Barrier integrity
Neurotransmitter production
Immune signaling
In developing children, where the gut–immune–brain axis is still maturing, these effects may be amplified.
Immune Activation Has a Metabolic Price
When the gut environment changes, the immune system responds.
Not always dramatically. Often quietly.
Low-grade immune activation still requires energy. It still requires resources. And it still competes with other biological priorities such as growth, repair, learning, and emotional regulation.
This is one reason symptoms that appear unrelated — fatigue, irritability, poor recovery, reduced resilience — often share a common underlying theme: energetic strain.
Mitochondria: The Overlooked Middle Layer
Mitochondria sit at the crossroads of:
Detoxification
Immune function
Neurological performance
Metabolic flexibility
When exposure load increases, mitochondrial efficiency can decrease — not catastrophically, but incrementally.
The result isn’t acute illness.
It’s reduced physiological margin.
Less buffer.
Less adaptability.
Less resilience.
Over time, that matters.
This Is Not About Fear — It’s About Formulation
This conversation is often mischaracterized as alarmist or anti-modern.
It shouldn’t be.
Preservatives are not inherently “bad.”
But they are biologically active.
And that means formulation choices matter.
The question is no longer:
“Can we use preservatives?”
It’s:
“Which ones, at what levels, in what combinations, and for whom?”
A developing child is not a scaled-down adult.
A chronically stressed system is not a resilient one.
A formulation optimized for shelf life is not automatically optimized for biology.
Why This Matters Beyond Food
This discussion extends well beyond packaged snacks.
It applies equally to:
Functional beverages
Nutritional supplements
Pediatric formulations
Clinical nutrition products
Ironically, many products designed to “support health” still rely on preservative strategies that increase biological load elsewhere.
That contradiction is becoming harder to justify.
A Systems Lens Changes the Conversation
When we view health through a systems lens, several things become clear:
No single ingredient explains complex outcomes
Cumulative exposure matters more than isolated thresholds
Energy availability is a limiting factor in resilience
Formulation is a biological decision, not just a technical one
This perspective doesn’t demand perfection.
It demands intentionality.
The Opportunity Ahead
As clinicians, formulators, and health innovators, we have an opportunity to do better — not by eliminating modern tools, but by using them more intelligently.
That means:
Reducing unnecessary additives where possible
Choosing preservative strategies with lower biological cost
Designing products that support, rather than tax, human systems
Convenience doesn’t have to come at the expense of resilience.
Clinical Implications of the New USDA Dietary Guidelines
The most recent USDA Dietary Guidelines have again raised concern that increasing animal-based protein intake may elevate cardiovascular disease (CVD) risk due to associated saturated fat consumption.
While this concern remains common, it is increasingly inconsistent with current cardiovascular research.
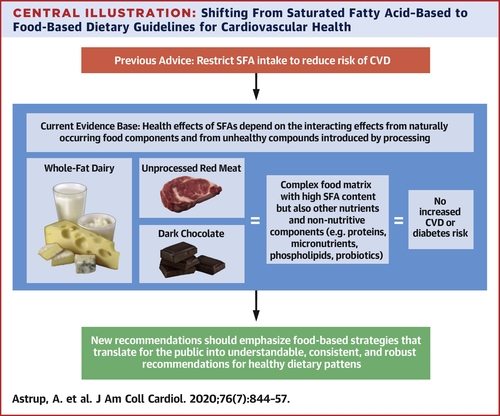
A comprehensive 2020 review published in the Journal of the American College of Cardiology—Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations—reexamined decades of epidemiologic, mechanistic, and interventional data. The authors concluded that saturated fat intake, in isolation, is a poor predictor of cardiovascular risk.
For clinicians, this distinction is highly relevant when interpreting dietary guidelines and counseling patients.
Limitations of LDL-C–Focused Risk Models
Current USDA guidance continues to emphasize saturated fat restriction largely through its impact on LDL cholesterol (LDL-C). However, the JACC review highlights a key limitation of this approach: LDL-C alone does not adequately reflect atherogenic risk.
More informative risk markers include:
LDL particle number and density
Insulin resistance and glycaemic regulation
Chronic inflammatory burden
Overall metabolic health status
Small, dense LDL particles—frequently associated with insulin resistance and hyperglycaemia—exhibit significantly greater atherogenic potential than large, buoyant LDL particles. Importantly, higher saturated fat intake within whole-food dietary patterns does not consistently produce this adverse lipid phenotype.
From a clinical standpoint, this challenges the assumption that saturated fat reduction should remain a primary target independent of metabolic context.
Historical Context and Policy Lag
The USDA’s continued caution regarding saturated fat reflects longstanding assumptions rooted in mid-20th-century observational research, particularly the Seven Countries Study led by Ancel Keys.
Subsequent evaluations have identified methodological limitations in this work, including selective data inclusion and insufficient control for confounding factors such as sugar intake, smoking prevalence, and lifestyle variables. More recent randomized trials and meta-analyses have not consistently replicated its conclusions.
Nevertheless, dietary policy has been slow to integrate newer mechanistic and clinical evidence.
Animal Protein: Clinically Relevant Distinctions
The USDA Dietary Guidelines largely categorize animal protein as a single entity. In clinical practice, this simplification obscures important distinctions.
Differences between:
CAFO-raised animal foods, and
Grass-fed, pasture-raised animal foods
extend beyond ethical considerations and include variations in fatty acid composition, micronutrient density, and inflammatory potential. These factors can meaningfully influence metabolic and inflammatory responses in patients.
Dietary Pattern and the Role of Fibre
Another limitation of saturated fat-focused guidance is the insufficient consideration of dietary pattern.
The JACC review emphasizes that saturated fat intake must be evaluated in conjunction with:
Fibre intake
Refined carbohydrate exposure
Insulin sensitivity and metabolic health
Dietary fibre plays a central role in insulin regulation, gut microbial ecology, bile acid metabolism, and lipid handling. When saturated fat is consumed within a fibre-rich, minimally processed dietary pattern, lipid changes commonly associated with increased cardiovascular risk are often attenuated or absent.
This context is rarely reflected in public dietary guidance but is highly relevant in individualized clinical care.
Practical Implications for Clinicians
For practitioners, the implication of the new USDA Dietary Guidelines is not that saturated fat should be universally promoted or avoided, but that single-nutrient targets are insufficient for cardiovascular risk assessment.
The most consistent drivers of CVD risk remain:
Insulin resistance
Chronic inflammation
Hyperglycaemia
Sedentary behavior
Ultra-processed food consumption
These factors are not caused by saturated fat intake alone and, in many cases, were exacerbated by decades of dietary guidance that encouraged refined carbohydrate substitution.
Conclusion
The renewed debate surrounding the USDA Dietary Guidelines highlights the need for a more physiologically grounded approach to cardiovascular nutrition—one that prioritizes metabolic health, dietary pattern, and food quality over isolated macronutrient thresholds.
The JACC review represents an important step toward that shift. For clinicians, incorporating this evidence into clinical reasoning may help reconcile public dietary policy with individualized patient care.
In Practice: Key Takeaways for Clinicians
Evaluate cardiovascular risk in the context of metabolic health, not LDL-C alone
Consider LDL particle characteristics, insulin resistance, and inflammation when assessing dietary fat intake
Distinguish between animal food sources rather than treating all animal protein as metabolically equivalent
Emphasize dietary pattern and fibre intake when discussing saturated fat with patients
Avoid reflexive fat restriction in metabolically healthy individuals without additional risk markers
Reference
Journal of the American College of Cardiology (2020)
Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations
Clinical Implications of the New USDA Dietary Guidelines
The most recent USDA Dietary Guidelines have again raised concern that increasing animal-based protein intake may elevate cardiovascular disease (CVD) risk due to associated saturated fat consumption.
While this concern remains common, it is increasingly inconsistent with current cardiovascular research.
A comprehensive 2020 review published in the Journal of the American College of Cardiology—Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations—reexamined decades of epidemiologic, mechanistic, and interventional data. The authors concluded that saturated fat intake, in isolation, is a poor predictor of cardiovascular risk.
For clinicians, this distinction is highly relevant when interpreting dietary guidelines and counseling patients.
Limitations of LDL-C–Focused Risk Models
Current USDA guidance continues to emphasize saturated fat restriction largely through its impact on LDL cholesterol (LDL-C). However, the JACC review highlights a key limitation of this approach: LDL-C alone does not adequately reflect atherogenic risk.
More informative risk markers include:
LDL particle number and density
Insulin resistance and glycaemic regulation
Chronic inflammatory burden
Overall metabolic health status
Small, dense LDL particles—frequently associated with insulin resistance and hyperglycaemia—exhibit significantly greater atherogenic potential than large, buoyant LDL particles. Importantly, higher saturated fat intake within whole-food dietary patterns does not consistently produce this adverse lipid phenotype.
From a clinical standpoint, this challenges the assumption that saturated fat reduction should remain a primary target independent of metabolic context.
Historical Context and Policy Lag
The USDA’s continued caution regarding saturated fat reflects longstanding assumptions rooted in mid-20th-century observational research, particularly the Seven Countries Study led by Ancel Keys.
Subsequent evaluations have identified methodological limitations in this work, including selective data inclusion and insufficient control for confounding factors such as sugar intake, smoking prevalence, and lifestyle variables. More recent randomized trials and meta-analyses have not consistently replicated its conclusions.
Nevertheless, dietary policy has been slow to integrate newer mechanistic and clinical evidence.
Animal Protein: Clinically Relevant Distinctions
The USDA Dietary Guidelines largely categorize animal protein as a single entity. In clinical practice, this simplification obscures important distinctions.
Differences between:
CAFO-raised animal foods, and
Grass-fed, pasture-raised animal foods
extend beyond ethical considerations and include variations in fatty acid composition, micronutrient density, and inflammatory potential. These factors can meaningfully influence metabolic and inflammatory responses in patients.
Dietary Pattern and the Role of Fibre
Another limitation of saturated fat-focused guidance is the insufficient consideration of dietary pattern.
The JACC review emphasizes that saturated fat intake must be evaluated in conjunction with:
Fibre intake
Refined carbohydrate exposure
Insulin sensitivity and metabolic health
Dietary fibre plays a central role in insulin regulation, gut microbial ecology, bile acid metabolism, and lipid handling. When saturated fat is consumed within a fibre-rich, minimally processed dietary pattern, lipid changes commonly associated with increased cardiovascular risk are often attenuated or absent.
This context is rarely reflected in public dietary guidance but is highly relevant in individualized clinical care.
Practical Implications for Clinicians
For practitioners and the general public, the implication of the new USDA Dietary Guidelines is not that saturated fat should be universally promoted or avoided, but that single-nutrient targets are insufficient for cardiovascular risk assessment.
The most consistent drivers of CVD risk remain:
Insulin resistance
Chronic inflammation
Hyperglycaemia (high blood sugar)
Sedentary behavior
Ultra-processed food consumption
These factors are not caused by saturated fat intake alone and, in many cases, were exacerbated by decades of dietary guidance that encouraged refined carbohydrate substitution.
Conclusion
The renewed debate surrounding the USDA Dietary Guidelines highlights the need for a more physiologically grounded approach to cardiovascular nutrition—one that prioritizes metabolic health, dietary pattern, and food quality over isolated macronutrient thresholds.
The JACC review represents an important step toward that shift. For clinicians, incorporating this evidence into clinical reasoning may help reconcile public dietary policy with individualized patient care.
In Practice: Key Takeaways for Clinicians
Evaluate cardiovascular risk in the context of metabolic health, not LDL-C alone
Consider LDL particle characteristics, insulin resistance, and inflammation when assessing dietary fat intake
Distinguish between animal food sources rather than treating all animal protein as metabolically equivalent
Emphasize dietary pattern and fibre intake when discussing saturated fat with patients
Avoid reflexive fat restriction in metabolically healthy individuals without additional risk markers
Reference
Journal of the American College of Cardiology (2020)
Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations
When discussing cardiovascular health, inflammation, or chronic disease risk, most conversations focus on cholesterol, blood pressure, or glucose. Yet one critical physiological factor is rarely discussed outside of advanced clinical and research settings: zeta potential.
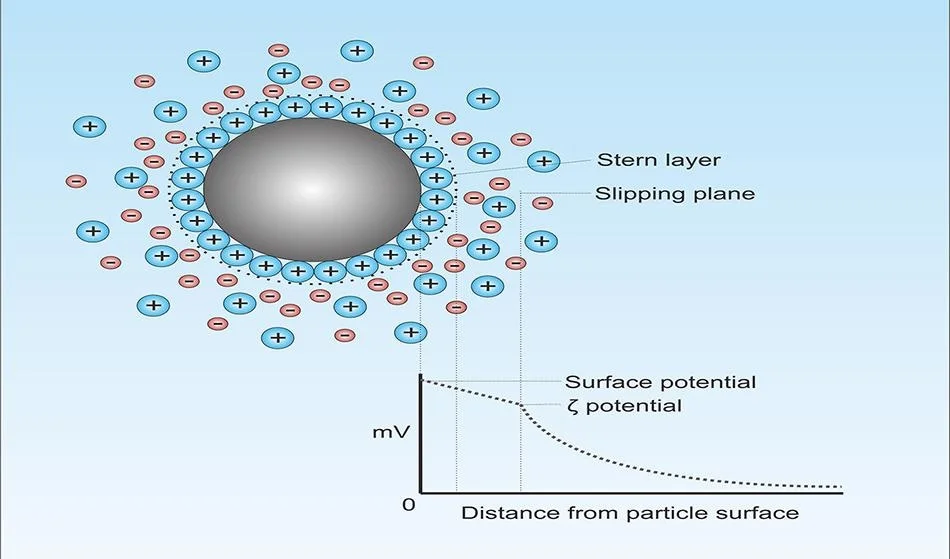
Zeta potential refers to the electrical charge on the surface of cells suspended in fluid, including red blood cells, platelets, and other circulating particles. This electrical charge determines whether cells repel each other and flow freely or clump together, impairing circulation.
What Is Zeta Potential?
Red blood cells naturally carry a negative surface charge. When this charge is strong, cells repel one another, maintaining proper spacing and allowing blood to flow smoothly through even the smallest capillaries.
When zeta potential is reduced, cells begin to aggregate (a phenomenon sometimes referred to as rouleaux formation). This increases blood viscosity, reduces microcirculation, and places greater strain on the cardiovascular system.
Why Zeta Potential Matters for Health
🔴 Acute Implications
Sluggish blood flow
Reduced oxygen and nutrient delivery
Increased clotting tendency
Impaired tissue perfusion during stress, illness, or dehydration
🔵 Chronic Implications
Persistently low zeta potential has been associated with:
Chronic inflammation
Cardiovascular disease risk
Hypertension
Metabolic dysfunction
Autoimmune and inflammatory conditions
Neurodegenerative processes linked to impaired cerebral circulation
Poor microcirculation can amplify metabolic chaos, where multiple physiological systems become stressed simultaneously rather than one isolated “root cause.”
What Lowers Zeta Potential?
Several common modern stressors reduce cellular charge and promote aggregation:
Chronic dehydration
High blood sugar and insulin resistance
Oxidative stress
Inflammatory cytokines
Poor electrolyte balance
Excess positively charged proteins and lipids
Chronic sympathetic (stress) dominance
Supporting Healthy Zeta Potential
Strategies that support cellular charge and blood flow include:
Adequate hydration with proper electrolytes
Supporting antioxidant status
Reducing inflammatory burden
Improving metabolic flexibility
Supporting liver and gut function (which influence plasma proteins)
Optimizing mineral balance
This systems-based approach improves flow, oxygen delivery, and cellular resilience rather than targeting isolated symptoms.
Why This Matters Clinically
Zeta potential provides insight into how well blood can actually deliver oxygen and nutrients, not just what appears on standard labs. It helps explain why some individuals experience fatigue, cold extremities, brain fog, or exercise intolerance despite “normal” conventional markers.
🔹 Work With Me
Formulation & Product Development
If your company or clinic is developing nutritional supplements or functional drinks, I provide consulting and formulation services to help create science-driven, evidence-based products that support circulation, metabolic resilience, and systemic health.
Clinical Support
If you’re struggling with ongoing symptoms and feel you’ve been told “everything looks normal,” I work with individuals using lab-informed, systems-based support to address metabolic chaos and restore physiological resilience.
Vitamin D has long been associated with bone density, immune balance, and calcium metabolism. Yet emerging research suggests its influence may extend much further—into the cellular mechanisms that govern how we age.
A newly published analysis from the VITAL trial, one of the most robust long-term randomized trials of nutrient supplementation to date, adds an important piece to the longevity conversation. The findings suggest that consistent Vitamin D₃ supplementation modestly but significantly preserved leukocyte telomere length over four years in older adults, compared with placebo.
This does not mean Vitamin D “stops aging.” But it does suggest that maintaining adequate Vitamin D status may help slow one measurable contributor to biological aging, particularly under conditions of metabolic and immune stress.
Telomeres: One Window Into Biological Aging
Telomeres are the protective caps at the ends of chromosomes. Each time a cell divides, telomeres shorten slightly. Over time, excessive shortening is associated with cellular senescence, impaired tissue repair, and increased disease vulnerability.
Telomere length is not destiny, nor is it the sole marker of aging. But it is a useful proxy for cumulative cellular stress—oxidative, inflammatory, immune, and metabolic.
In the VITAL sub-study, participants receiving Vitamin D₃ (2,000 IU/day) experienced significantly less telomere shortening than those receiving placebo. Omega-3 fatty acids, notably, did not show the same effect in this analysis.
The magnitude of benefit was described as modest but statistically significant, which is exactly what we expect from nutritional interventions that support physiology rather than override it.
Why Vitamin D May Matter in a Metabolic Chaos™ Context
From a functional and Metabolic Chaos™ lens, aging is not driven by a single “root cause,” but by interacting stressors that accumulate over time:
Immune dysregulation
Chronic low-grade inflammation
Mitochondrial inefficiency
Impaired DNA repair
Circadian disruption
Reduced hormonal signaling resilience
Vitamin D intersects with many of these systems simultaneously:
Immune modulation (innate and adaptive balance)
Inflammation signaling control
Mitochondrial gene expression
Genomic stability and DNA replication fidelity
Calcium signaling beyond bone tissue
Rather than acting as an anti-aging “switch,” Vitamin D appears to function more like a system stabilizer—helping cells respond more appropriately to ongoing stress.
In other words, it may help reduce the rate at which Metabolic Chaos accumulates.
No Megadoses, No Biohacking Extremes
One of the most important aspects of the VITAL findings is what wasn’t used:
No megadoses
No aggressive protocols
No pharmacologic intervention
Participants followed consistent, physiologic dosing over years—not weeks—and still demonstrated measurable benefit.
This reinforces a critical principle in functional and nutritional medicine:
Longevity support is often about consistency, sufficiency, and system support—not intensity.
Who Is Most Likely to Benefit?
Vitamin D insufficiency remains common, particularly in individuals who:
Spend most of their time indoors
Live at northern or southern latitudes
Have darker skin pigmentation
Experience chronic stress or immune activation
Carry higher body fat percentages
In clinical and practitioner settings, Vitamin D status often correlates with immune load, inflammatory tone, and recovery capacity rather than symptoms alone.
This is why testing—not guessing—is essential.
Practical Considerations (General Education Only)
Always assess serum 25-hydroxyvitamin D levels before long-term supplementation
Many adults fall into a maintenance range with 2,000–4,000 IU/day, though individual needs vary
Vitamin D works synergistically with Vitamin K₂, magnesium, and adequate dietary fat
Sun exposure, lifestyle stress, sleep, and gut absorption all influence outcomes
Vitamin D should be viewed as one contributor within a broader systems strategy, not a stand-alone solution.
Aging Is Not Just About Time
Chronological aging is inevitable. Biological aging is variable.
Cellular resilience, repair capacity, and immune balance determine how well we adapt to stress over time. Vitamin D appears to support these processes quietly, incrementally, and safely when used appropriately.
Not a miracle. Not a cure. But potentially a meaningful support lever for long-term cellular health.
Scientific Reference
Zhu H, et al. Vitamin D₃ supplementation, but not omega-3 fatty acids, preserves leukocyte telomere length over 4 years in older adults: results from the VITamin D and OmegA-3 TriaL (VITAL).The American Journal of Clinical Nutrition. 2025;121(6):1720-1731. Findings demonstrate modest but statistically significant benefits and warrant further replication.
Work With Me
I work with clinics, practitioners, and health-focused companies to design evidence-aligned nutritional supplement and functional drink formulations, and to help individuals understand how multiple physiological contributors interact over time.
I’m honored to share that I have joined First Compounding Pharmacy Limited (FCPL) in Nairobi, Kenya as Chief Operations Officer & Head of Compounding Formulation.
This role marks a major milestone in my career and an unprecedented opportunity to help transform healthcare across Kenya and the broader East African region.
Why This Work Matters
Many of the tools we take for granted in North America — ✓ personalized formulations ✓ pharmaceutical-grade compounding services ✓ bioidentical hormone preparations ✓ functional & integrative medicine training ✓ nutrition-based metabolic assessment — are not yet widely available in East Africa.
At FCPL, we are changing that.
Our mission is to introduce world-class, evidence-based compounding and integrative healthcare solutions that will dramatically expand what is possible for clinicians and their patients throughout the region.
My Role at FCPL
As COO and Head of Compounding Formulation, I will be leading:
Compounding formulation (sterile & non-sterile) Development of a 46-SKU botanical precision-medicine range Operational systems & quality assurance integration Practitioner education programs in functional nutrition, integrative medicine, and metabolic assessment Clinical translation of regenerative and longevity protocols
My goal is to help build the most advanced compounding and integrative health platform in East Africa, setting new standards for safety, efficacy, and patient outcomes.
Background & Experience I Bring to This Role
With more than 15 years in functional medicine, nutritional biochemistry, lab-based assessment, and formulation science, my work has included:
• Master nutraceutical formulation for Healthspan Formulations and Cell Factors Regenerative Medicine • Leading development of next-generation metabolic and regenerative formulations • Thousands of clinical assessments using arterial pulse wave velocity, bioimpedance, and functional blood chemistry • Teaching roles at Boucher Naturopathic Medical School (Vancouver) • Building multimillion-dollar clinical distribution and education programs • Training hundreds of practitioners across North America in functional and integrative frameworks
This new chapter allows me to apply that experience toward building healthcare capacity where it is needed most.
A Transformational Opportunity for Kenya & East Africa
FCPL represents the first large-scale initiative to bring:
• Compounding pharmacy services • Bioidentical hormone options • Evidence-based botanical formulations • Functional nutrition training • Integrative oncology support • Dietary metabolic typing and personalized nutrition
…into a region where these services are just beginning to emerge.
It is a privilege to help lead this effort.
Thank You
I’m deeply grateful to everyone who supported my professional journey and encouraged me to pursue meaningful, high-impact work around the world.
I look forward to collaborating with clinicians, researchers, and partners across Kenya and East Africa to advance a new standard of personalized, integrative healthcare.
The Environmental Working Group (EWG) is a nonprofit research and advocacy organization dedicated to empowering consumers with evidence-based tools to reduce environmental exposures. Their Dirty Dozen Guide to Food Chemicals highlights 12 additives and contaminants that contribute significantly to dietary chemical load.
In the context of the Metabolic Chaos™ Blueprint, these exposures represent contributors to total stress load—not root causes—affecting digestion, hormones, detoxification, mitochondria, and inflammatory pathways.
The Official EWG “Dirty Dozen” Food Chemicals
(As listed on the 2025 EWG guide)
Nitrites and nitrates
Propyl paraben
Brominated vegetable oil (BVO)
Titanium dioxide
BHA (butylated hydroxyanisole)
BHT (butylated hydroxytoluene)
Azodicarbonamide (ADA)
Potassium bromate
TBHQ (tert-butylhydroquinone)
Artificial colors (Red 40, Yellow 5, etc.)
PFAS in food packaging
Perchlorate
Each of these compounds has been evaluated for endocrine disruption, mitochondrial stress, inflammatory activation, or digestive burden—key nodes within the Metabolic Chaos™ physiological network.
Why These Chemicals Matter (Metabolic Chaos™ Clinical Lens)
• They add to the body’s total physiological load
Chronic exposure increases metabolic demand on liver detox pathways (Phase I–III), bile flow, and antioxidant reserves.
• They influence hormonal communication
Parabens, nitrates, and synthetic dyes can modulate pathways linked to the HPA axis, estrogen activity, or stress responses.
• They burden digestion and the gut microbiome
Titanium dioxide and persistent PFAS residues may disrupt gut lining integrity and microbiome balance.
• They promote systemic inflammation
BHA, BHT, and TBHQ may elevate oxidative stress, triggering immune activation and inflammatory signaling.
In FDN methodology, we avoid “root cause” narratives and instead understand that these compounds contribute to a terrain of dysfunction when combined with stress, poor sleep, blood sugar instability, nutrient deficiencies, and environmental toxins.


 Compounding formulation (sterile & non-sterile)
Compounding formulation (sterile & non-sterile) Development of a 46-SKU botanical precision-medicine range
Development of a 46-SKU botanical precision-medicine range Operational systems & quality assurance integration
Operational systems & quality assurance integration Practitioner education programs in functional nutrition, integrative medicine, and metabolic assessment
Practitioner education programs in functional nutrition, integrative medicine, and metabolic assessment Clinical translation of regenerative and longevity protocols
Clinical translation of regenerative and longevity protocols